

[vc_row type=”in_container” full_screen_row_position=”middle” column_margin=”default” column_direction=”default” column_direction_tablet=”default” column_direction_phone=”default” scene_position=”center” text_color=”dark” text_align=”left” row_border_radius=”none” row_border_radius_applies=”bg” overlay_strength=”0.3″ gradient_direction=”left_to_right” shape_divider_position=”bottom” bg_image_animation=”none”][vc_column column_padding=”no-extra-padding” column_padding_tablet=”inherit” column_padding_phone=”inherit” column_padding_position=”all” column_element_spacing=”default” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” gradient_direction=”left_to_right” overlay_strength=”0.3″ width=”1/1″ tablet_width_inherit=”default” tablet_text_alignment=”default” phone_text_alignment=”default” bg_image_animation=”none” border_type=”simple” column_border_width=”none” column_border_style=”solid”][vc_column_text]When an incident happens, the primary approach to incident analysis is root cause analysis (RCA). To understand and prevent the recurrence of incidents that cause or have the potential to cause safety-related failures, we know we must analyze such incidents rigorously and systemically. Such a process typically walks you through recognition of incident root causes to establish workable hazard mitigation solutions.
The issue with many traditional root cause analysis systems is a focus on the identification of one underlying primary cause. In Hile Group’s experience when conducting root cause analysis, there is never one root, but rather multiple causes that together generate an environment ripe for the incident to occur.
Systems that focus on one root cause analysis are vulnerable to the narrow development of corrective actions, potentially leaving latent, unidentified hazards within the system. Through our 30 years of safety culture work, Hile Group developed its proprietary system, Multiple Cause Incident Analysis or MCIA as a more thorough and complete solution to preventing recurrence of catastrophic incidents and injuries.
Through Hile Group’s proven MCIA system, each identified gap in safety performance has much to teach us about how we might effectively manage risk. Grasping the multiple factors that contribute to error can lead to strategic, targeted systems fixes—the right fixes the first time.
Certainly, in the process of understanding gaps in safety performance using traditional Root Cause Analysis, we have all seen pitfalls such as:
- Focus on the specific incident’s circumstances – bad apple theory
- Methodology not structured in a way to prevent bias
- Analysis centers around employee and equipment fault and fixes
- Flawed definition of the initial gap, driven by an incident analysis team’s unchecked assumption
- Fear of blame on the part of any stakeholder whose actions might in some way be interpreted as contributing to the incident
- The desire for one clean, simple, concrete solution to the problem—sometimes exacerbated by the notion that we seek a single “root” cause
Benefits of MCIA
- Documents safety-related problem solving reliably and objectively, significantly reducing the guess work involved in “getting to the bottom of things”
- Framework guides analysis to telescope out and see the big picture of the incident, combating hindsight bias
- Agreement on root causes and on prioritization of the countermeasures that address these key causes sharpens focus on the corrective actions likely to have the greatest long-term impact
- Brings a system to the table that is thorough, unbiased, and supports a safety culture based in preventive solutions
- Provides the ability for a large organization to learn across multiple sites/facilities. The methodology was designed to help identify systemic flaws in process/policy/procedure that, after identified in one situation, can be implemented across the organization to avoid similar incidents everywhere.
- Guides team members to understand multiple causation and to share the responsibility for closing known safety performance gaps
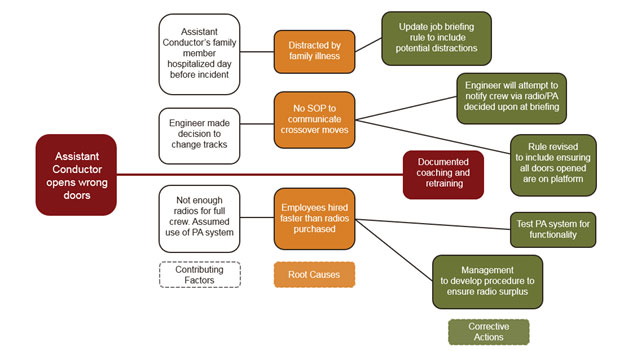
A Case Study of Root Cause Analysis vs. Multiple Cause Incident Analysis
In the below examples, you will see a sample case worked through both systems. While they both begin with the same incident involving a train conductor, the traditional root cause analysis focuses on the involved employee as the primary cause, whereas MCIA takes into consideration factors such as equipment limitations, supervisory decisions, and outside influences. You’ll note very different conclusions and Corrective Actions with both systems. The traditional model recommends a narrowed solution that only applies to the current situation, yet MCIA proposes solutions that will not only resolve the situation, but address and remedy gaps in the entire system.
Root Cause Analysis

MCIA
MCIA reality checks its system-level data collection and contributing factor identification by including multi-stakeholder teams whose combined perspective deters “blame the victim” or “hindsight bias,” increasing the likelihood that Corrective Actions will hit their targets the first time and for good![/vc_column_text][/vc_column][/vc_row]
